
This is a well documented injury resulting from improperly injected vaccines (not just covid, any vaccine). It even has an acronym: SIRVA (Shoulder injury related to vaccine administration).
Shoulder injury related to vaccine administration is an under-reported, preventable series of events caused by incorrect technique or landmarking for intramuscular deltoid injections.1,2 Specifically, SIRVA occurs when an intramuscular deltoid injection is administered into the shoulder joint.1,2 This results in an inflammatory process that causes damage to the musculoskeletal structures including the bursae, tendons, and ligaments.2 The main symptoms include persistent shoulder pain and a limited range of motion.2 The keys to distinguishing SIRVA are that the symptoms typically begin within 48 hours of vaccine administration and that they do not improve with over-the-counter analgesic medications.2 Patients will often visit their physicians months later because they are not able to carry out daily tasks that were possible before the vaccination.2 These patients are often diagnosed with inflammatory injuries such as bursitis, rotator cuff tears, and adhesive capsulitis.1,2 During physical examination and on ultrasound scan, SIRVA will not appear to be any different from routine shoulder injuries. The only difference is that the shoulder symptoms will have started within days of a vaccination. Thus, shoulder injury related to vaccine administration is a term that describes improper landmarking of vaccinations that results in shoulder injuries such as adhesive capsulitis or bursitis. Treatment for SIRVA is the same as treatment for routine inflammatory injuries.1,2
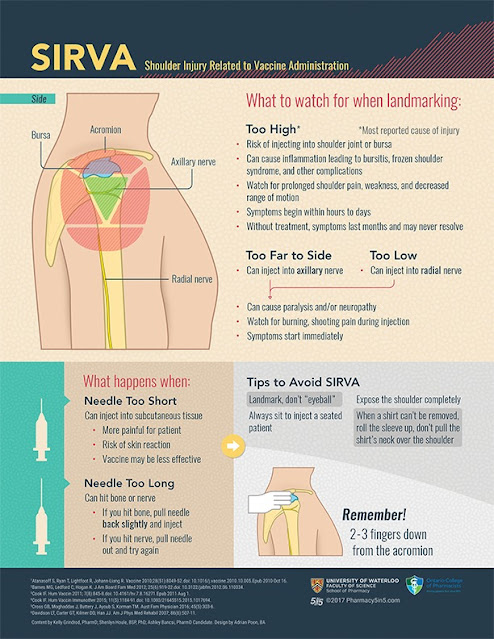
While the prevalence of SIRVA in Canada is unknown, as it is under-reported,1 the global increase in case reports demonstrates that SIRVA is a developing topic. There is little information on the types of vaccines most likely to cause SIRVA, although case reports have been published on many different types of intramuscular vaccines. Primary care providers are well positioned to prevent injury through proper injection technique and by recognizing, diagnosing, and offering treatment to patients with SIRVA. We developed an infographic (Figure 1), also available at CFPlus,* to guide all health professionals in proper injection administration and the prevention of SIRVA. To develop the infographic and accompanying article, we performed a literature search using terms related to SIRVA (shoulder injury related to vaccine administration, incorrect vaccine administration, bursitis, and frozen shoulder), its causes (improper landmarking and incorrect deltoid injection), and other injection site events (radial nerve injury, axillary nerve injury, nodules, and cellulitis) in the PubMed, EMBASE, and Google Scholar databases.
Other injection site events
Case reports that mention SIRVA also describe other shoulder injuries that can occur when landmarking is not performed correctly. Injections that occur below the deltoid muscle can hit the radial nerve and injections that are too far to the side of the deltoid muscle can hit the axillary nerve.3,4 If a nerve is hit, the patient will feel an immediate burning pain, which can result in paralysis or neuropathy that does not always resolve.3,4
Importance of needle length
Needle length should be chosen based on the body habitus and weight of the patient.5 A needle that is too long can penetrate the deltoid muscle, hitting the bone.4 Although patients will not feel their bones being hit, the vaccine might not fully absorb into the muscle, leading to a reduced immune response.4 Furthermore, if the needle is too short the vaccine might be administered subcutaneously, which might result in decreased immune response and the development of nodules or cellulitis.4
The efficacy of vaccines administered outside the proper injection site is not guaranteed or quantified. In particular, a 16-mm (5/8-inch) needle should be chosen for patients weighing less than 60 kg (130 lb) and a 25-mm (1-inch) needle is appropriate for patients weighing 60 to 70 kg (130 to 152 lb).5 Women weighing 70 to 90 kg (152 to 200 lb) or men weighing 70 to 118 kg (152 to 260 lb) should receive injections with either a 25-mm (1-inch) or 38-mm (1.5-inch) needle.5 A 38-mm (1.5-inch) needle is necessary for women weighing more than 90 kg (200 lb) and men weighing more than 118 kg (260 lb).5 All health care professionals who provide injections should make individualized needle length selection part of their injection administration routine.
Conclusion
The key to preventing SIRVA and other vaccine injuries is to always use landmarking. The next time
you give a vaccine to a patient, pay attention to your technique. Even the most experienced health care professionals can develop bad habits and need to polish their skills periodically.









