
Showing posts with label Remdesirvir. Show all posts
Showing posts with label Remdesirvir. Show all posts
15 things everyone needs to know about COVID and how to treat it

- Avoid all the COVID vaccines, even Novavax. Just say no. It’s not for anyone. No exceptions. The data show that these vaccines kill more people than they save. You can end up dead or disabled or with a compromised immune system for the rest of your life. For kids, for example, we will kill over 100 kids to save 1 life from COVID. These are the most dangerous vaccines ever deployed; 800x more deadly than the smallpox vaccine. Novavax has a much better safety profile than the current vaccines, but there may be serious, longer term risks here that we need to quantify. It’s not their fault… the spike protein is particularly toxic because it was designed to be toxic (I’m friends with Li-Meng Yan; we talk). The experts I work with say “not enough data.” So our advice is let’s wait for the data and use early treatment in the meantime. You can never unvaccinate yourself and right now early treatments are a great solution with higher efficacy and known safety.
- If you get COVID, start early treatment ASAP as soon as you have symptoms. Early treatment is much safer and there is a much lower chance of long haul COVID, MIS-C, and adverse events. See my treatment advice for details; many options are available without a doctor or prescription. The immunity you acquire from getting the real virus is both robust and durable.
- Make sure you have your early treatment drugs already in your house so you can start treatment as soon as you have symptoms.
- If you aren’t sure you have COVID, you can get a PCR test, but these can be inaccurate. If you have symptoms, you can use a home test kit such as the binax now kit (Note: they will not work unless you currently are symptomatic, so don’t use these kits for employer screening; it’s a complete waste of money).
- The mainstream media wants to keep you in the dark about the truth about these vaccines so they only tell you one side of the story and they censor competent speakers on the other side. This is why you will never see Peter McCullough on CNN, in the NY Times, etc. They will never sponsor a debate between the top experts on both sides because that would destroy the false narrative and damage the reputation of the mainstream media. So they have to tell only one side of the narrative.
- The whole pandemic response was unnecessary. The lockdowns, social distancing, masking, business restrictions, etc. We knew back in March 2020 that a cocktail of repurposed drugs given early could keep people out of the hospital and turn COVID into a mild cold with no long-term side effects.
- The NIH is deliberately suppressing early treatments that work like fluvoxamine, ivermectin, vitamin D, inhaled budesonide, etc. Even after fluvoxamine was proven in a large Phase 3 clinical trial with an incredible 12X reduction in hospitalization, the NIH did nothing. Absolutely nothing. They do not want you to know about fluvoxamine. When Fareed and Tyson tried to get the NIH and FDA’s attention in March 2020 on their protocol which has a 99.76% risk reduction (better than anything else), they were ignored.
- Masks don’t work. It is political theater to prove they can use fear to get you to do nonsensical things. Nobody will debate my team on this because it would destroy their argument.
- Never trust the CDC, FDA, NIH, and medical community again. This is the most dangerous vaccine in human history and the CDC couldn’t find a single safety signal (it was the DoD that spotted myocarditis). The NIH is sand-bagging early treatment. The mainstream medical community is basically believing everything the FDA and CDC are telling them without bothering to double-check anything.
- Avoid the hospital. If you do get hospitalized, refuse intubation and remdesivir. Get a court order to get cyproheptadine, fluvoxamine, and/or ivermectin. You will need a court order because all hospitals will refuse these proven treatments. See the list of hospitalized treatment protocols.
- They could end vaccine hesitancy worldwide anytime they wanted. All they have to do is agree to a single 3 hour debate. But none of the so-called experts who claim the vaccines are safe will debate our team. This is because they know they will lose. So they must ignore and censor us. Their unwillingness to have a fair scientific discussion with experts on both sides tells you everything you need to know about who has the better argument.
- If you maintain very high levels of Vitamin D, you can greatly reduce your chance of getting sick from COVID. It’s the simplest thing to do and it is safe and effective. There’s a strong correlation between your vitamin D level and your risk of dying from COVID-19. At a level of 17 ng/mL, the death rate is nearly 100%. At a level of 35 ng/mL, the death rate is near zero. It is inexplicable that the medical community and/or NIH isn’t telling people this.
- Fluvoxamine is highly effective if you get COVID. The best dose is 50mg twice a day for 14 days. Take it as soon as you have symptoms. The side effect profile is near zero as long as you avoid coffee. If you can’t get fluvoxamine, you can use 30mg once a day of fluvoxetine. Both drugs work for hospitalized patients as well. Many other drugs are very effective. See my treatment advice for details.
- The single best drug if you get COVID is Interferon Lambda, but it is not FDA approved; it is available only in clinical trials. It works because it replaces the interferon that the virus disables when it attacks you. D-dimer is greatly reduced in the treatment group… this is very telling.
- The reason all this happened is that people don't double-check authorities. They believe the authorities, and it creates a domino effect. They aren't inherently evil, just trusting the wrong people. They think I'm an evil person because I disagree with the authorities. I disagree because the data doesn’t support what we are being told. Few people (especially doctors) have the time/expertise to understand/analyze VAERS. We haven't found *anyone* in the world who is able to "correct" our calculation. But as long as people think we are misinformation spreaders, nobody listens to us. Most people will make decisions based on the # of “experts” supporting a viewpoint, not by looking at the data directly; few people have the time and expertise to do that. I did that in early May, 2021 and here is the first article I wrote at the time (Should you get vaccinated?) after I was convinced the vaccines were causing harm. I lost a lot of friends after writing that article, but it was the right thing to do and I don’t regret it. I think I’ve made more than 100X new friends by standing up for science and truth. I also found a very odd asymmetry… everyone on our side will happily engage the other side in a discussion on the merit, but not vice versa. They just want to tell us we are wrong, but will not explain to us why we are wrong (since they don’t know).
Doctor With Natural Immunity Fired For Fefusing Vaccine & Using Ivermectin
St. Louis ICU physician - who fought the COVID-19 pandemic on the front lines for 18 months - is out of a job after refusing to get the COVID-19 vaccine.
A local ICU physician – who fought the Covid pandemic on the front lines for 18 months – is out of a job after refusing to get the vaccine.
Dr. Mollie James said she was employed at two health systems in the Midwest, including in St. Louis, for much of the pandemic. She was also splitting her time between local hospitals and one in New York.
James has worked as a trauma and acute care surgeon for 11 years, four of which were spent in St. Louis.
“When the pandemic hit I just felt a calling to go to New York when they called for volunteers,” she said. “So I went there in April of 2020 and I liked being in the midst of it. My purpose for going was to help them out, but also to see what they were doing in real time and what was the most effective for patients so I could bring that back to the community.”
For most of the last year and a half, James said she traveled between New York and St. Louis, working with critical ICU patients infected with COVID-19 in multiple hospitals.
“I was scared, so I have a lot of empathy for the people who live in fear, because we didn’t know,” she said. “About that time nurses were dying. Doctors were dying. And so I didn’t know what we were getting into.”
James said she tested positive for Covid in March of 2020, about a month before volunteering to go to New York. Still, she said she was nervous. “We had freezer trucks serving as morgues outside my hospital so it was a very real reminder to wear all of the personal protective gear,” she said.
During her time treating patients at the height of the pandemic, James said one of the first big improvements in treatment she witnessed was the addition of steroids and blood thinners to treatment protocols.
In December of 2020, James said the Senate testimony of Dr. Pierre Kory, a fellow ICU physician, caught her eye.
“He started talking about Ivermectin,” she said. “At the time, I wasn’t familiar with that medication, so I started looking into it and the dosing protocols and the side effects and the downsides to it. We started slowly using it in a few patients, then the pandemic numbers went down and I didn’t really see a big difference at that time.”
When a surge of Covid cases hit southwest Missouri, James said she started doing additional research on the drug and the concept of early outpatient treatment.
“There’s an entire protocol and Ivermectin is a key part of it. We use blood thinners and different vitamins along with a stronger steroids than most people use, called Methylprednisolone. We combine that with Ivermectin and that combination seems to be extremely effective.”
“I had two patient successes at the hospital that was offering it and they pulled it off the shelf a week later,” James said. “I was told it wasn’t approved by the COVID committee so doctors who were not involved in the patient’s care, my patient’s care, were making decisions about what I could use.”
Dr. Clay Dunagan, the head of the St. Louis Metropolitan Pandemic Task Force, looked into James’ claims but said there are better treatment options available. “It’s conceivable that Ivermectin has some impact early in the disease but it’s not really something we should be using. We have other drugs that are more effective,” he said.
Dunagan said early data shows Ivermectin doesn’t make much of a difference and he believes Remdesivir, an anti-viral drug, along with other steroids benefit patients more.
James said the decision should be between a patient and their doctor.
“When I was able to properly dose and use Ivermectin in an ICU patient, I saw the fastest turnaround of any patient out of probably a couple thousand that I’ve treated,” James said.
“When you have administrators telling physicians what medications they can prescribe, or how to counsel patients regarding interventions or telling them not to do something they believe is in the patient’s best interest, I think doctors have an obligation to leave those situations.”
Because James recovered from COVID-19, she believes her natural immunity outweighs any medical need for a vaccine. She said she doesn’t actively encourage her patients to get vaccinated, but did add she believes it’s a decision that should ultimately be left up to a patient and their doctor.
James admits her position on the use of Ivermectin and vaccination status places her in the minority of healthcare workers. Still, she said she’s speaking out based on the tragedy she’s witnessed firsthand.
“I think there are a lot of people living in fear, they’ve been sold fear for a long time. They don’t need to be afraid, they just need to be informed,” James said. “They need to arm themselves with the knowledge and potentially the medications so they know what to do and get back to life.”
James is in private practice now, seeing patients virtually from across the country. She said she will prescribe several medications, including Ivermectin, to patients who have tested positive.
“Everyone is a candidate for early treatment. I believe its 85 percent effective in keeping people out of the hospital.”
She adds she’s run into roadblocks at pharmacies, with pharmacists unwilling to fill prescriptions for Ivermectin. Insurance companies don’t cover it either, leaving patients to pay out-of-pocket.
Almost 50% of Hospitalized with COVID-19 Had Mild or Asymptomatic Cases
div class="separator" style="clear: both; text-align: center;">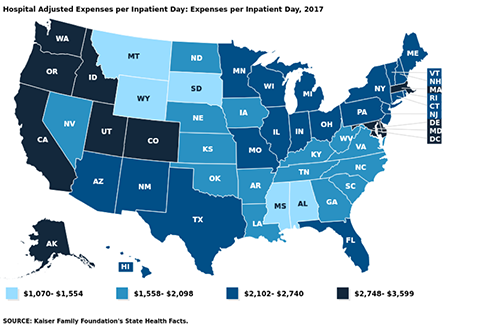

US hospitals typically spend $2,424/day to provide inpatient care. Are hospitalizations another federal money grab?

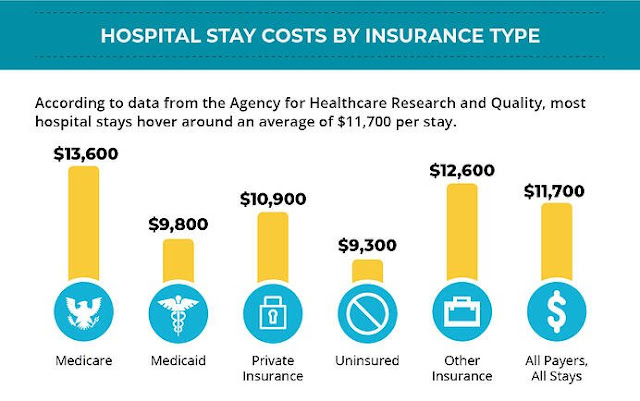
Hospital Stay Costs by Insurance Type
A new study suggests that almost half of those hospitalized with COVID-19 have mild or asymptomatic cases.
Researchers from Harvard Medical School, Tufts Medical Center, and the Veterans Affairs Healthcare System took on the task of trying to figure out how serious Covid cases were in those hospitalized, and how many people counted as Covid hospitalizations were actually in the hospital for Covid, versus getting a Covid test after being admitted for something else.
The study "analyzed the electronic records for nearly 50,000 COVID hospital admissions at the more than 100 VA hospitals across the country," The Atlantic wrote. It "checked to see whether each patient required supplemental oxygen or had a blood oxygen level below 94 percent" in order to try and determine if cases met the NIH's threshold for "severe COVID".
What the study found was that from March 2020 to January 2021, 36% of Covid cases in the hospital were mild or asymptomatic. From January 2021 to June 2021, during the Delta variant's spread, that number rose all the way to 48%. For vaccinated hospital patients, the number rose to a stunning 57%.
At least 12,000 Americans have already died from COVID-19 this month, as the country inches through its latest surge in cases. But another worrying statistic is often cited to depict the dangers of this moment: The number of patients hospitalized with COVID-19 in the United States right now is as high as it has been since the beginning of February. It’s even worse in certain places: Some states, including Arkansas and Oregon, recently saw their COVID hospitalizations rise to higher levels than at any prior stage of the pandemic. But how much do those latter figures really tell us?
From the start, COVID hospitalizations have served as a vital metric for tracking the risks posed by the disease. Last winter, this magazine described it as “the most reliable pandemic number,” while Vox quoted the cardiologist Eric Topol as saying that it’s “the best indicator of where we are.” On the one hand, death counts offer finality, but they’re a lagging signal and don’t account for people who suffered from significant illness but survived. Case counts, on the other hand, depending on which and how many people happen to get tested. Presumably, hospitalization numbers provide a more stable and reliable gauge of the pandemic’s true toll, in terms of severe disease. But a new, nationwide study of hospitalization records, released as a preprint today (and not yet formally peer-reviewed), suggests that the meaning of this gauge can easily be misinterpreted—and that it has been shifting over time.
If you want to make sense of the number of COVID hospitalizations at any given time, you need to know how sick each patient actually is. Until now, that’s been almost impossible to suss out. The federal government requires hospitals to report every patient who tests positive for COVID, yet the overall tallies of COVID hospitalizations, made available on various state and federal dashboards and widely reported on by the media, do not differentiate based on the severity of illness. Some patients need extensive medical intervention, such as getting intubated. Others require supplemental oxygen or administration of the steroid dexamethasone. But there are many COVID patients in the hospital with fairly mild symptoms, too, who have been admitted for further observation on account of their comorbidities, or because they reported feeling short of breath. Another portion of the patients in this tally are in the hospital for something unrelated to COVID, and discovered that they were infected only because they were tested upon admission. How many patients fall into each category has been a topic of much speculation. In August, researchers from Harvard Medical School, Tufts Medical Center, and the Veterans Affairs Healthcare System decided to find out.
Researchers have tried to get at similar questions before. For two separate studies published in May, doctors in California read through several hundred charts of pediatric patients, one by one, to figure out why, exactly, each COVID-positive child had been admitted to the hospital. Did they need treatment for COVID, or was there some other reason for admission, like cancer treatment or a psychiatric episode, and the COVID diagnosis was merely incidental? According to the researchers, 40 to 45 percent of the hospitalizations that they examined were for patients in the latter group.
The authors of the paper out this week took a different tack to answer a similar question, this time for adults. Instead of meticulously looking at why a few hundred patients were admitted to a pair of hospitals, they analyzed the electronic records for nearly 50,000 COVID hospital admissions at the more than 100 VA hospitals across the country. Then they checked to see whether each patient required supplemental oxygen or had a blood oxygen level below 94 percent. (The latter criterion is based on the National Institutes of Health definition of “severe COVID.”) If either of these conditions was met, the authors classified that patient as having moderate to severe disease; otherwise, the case was considered mild or asymptomatic.
The study found that from March 2020 through early January 2021—before vaccination was widespread, and before the Delta variant had arrived—the proportion of patients with mild or asymptomatic disease was 36 percent. From mid-January through the end of June 2021, however, that number rose to 48 percent. In other words, the study suggests that roughly half of all the hospitalized patients showing up on COVID-data dashboards in 2021 may have been admitted for another reason entirely, or had only a mild presentation of the disease.
This increase was even bigger for vaccinated hospital patients, of whom 57 percent had mild or asymptomatic disease. But unvaccinated patients have also been showing up with less severe symptoms, on average, than earlier in the pandemic: The study found that 45 percent of their cases were mild or asymptomatic since January 21. According to Shira Doron, an infectious-disease physician and hospital epidemiologist at Tufts Medical Center, in Boston, and one of the study’s co-authors, the latter finding may be explained by the fact that unvaccinated patients in the vaccine era tend to be a younger cohort who are less vulnerable to COVID and may be more likely to have been infected in the past.
Among the limitations of the study is that patients in the VA system are not representative of the U.S. population as a whole, as they include few women and no children. (Still, the new findings echo those from the two pediatric-admissions studies.) Also, like many medical centers, the VA has the policy to test every inpatient for COVID, but this is not a universal practice. Lastly, most of the data—even from the patients admitted in 2021—derived from the phase of the pandemic before Delta became widespread, and it’s possible that the ratios have changed in recent months. The study did run through June 30, however, when the Delta wave was about to break, and it did not find that the proportion of patients with moderate to severe respiratory distress was trending upward at the end of the observation period.
The idea behind the study and what it investigates is important, says Graham Snyder, the medical director of infection prevention and hospital epidemiology at the University of Pittsburgh Medical Center, though he told me that it would benefit from a little more detail and nuance beyond oxygenation status. But Daniel Griffin, an infectious disease specialist at Columbia University, told me that using other metrics for the severity of illness, such as intensive-care admissions, presents different limitations. For one thing, different hospitals use different criteria for admitting patients to the ICU.
One of the important implications of the study, these experts say, is that the introduction of vaccines strongly correlates with a greater share of COVID hospital patients having mild or asymptomatic disease. “It’s underreported how well the vaccine makes your life better, how much less sick you are likely to be, and less sick even if hospitalized,” Snyder said. “That’s the gem in this study.”
“People ask me, ‘Why am I getting vaccinated if I just end up in the hospital anyway?’” Griffin said. “But I say, ‘You’ll end up leaving the hospital.’” He explained that some COVID patients are in for “soft” hospitalizations, where they need only minimal treatment and leave relatively quickly; others may be on the antiviral drug remdesivir for five days, or with a tube down their throat. One of the values of this study, he said, is that it helps the public understand this distinction—and the fact that not all COVID hospitalizations are the same.
But the study also demonstrates that hospitalization rates for COVID, as cited by journalists and policymakers, can be misleading, if not considered carefully. Clearly many patients right now are seriously ill. We also know that overcrowding of hospitals by COVID patients with even mild illness can have negative implications for patients in need of other care. At the same time, this study suggests that COVID hospitalization tallies can’t be taken as a simple measure of the prevalence of severe or even moderate disease, because they might inflate the true numbers by a factor of two. “As we look to shift from cases to hospitalizations as a metric to drive policy and assess the level of risk to a community or state or country,” Doron told me, referring to decisions about school closures, business restrictions, mask requirements, and so on, “we should refine the definition of hospitalization. Those patients who are there with rather than from COVID don’t belong in the metric.”
Among the limitations of the study is that patients in the VA system are not representative of the U.S. population as a whole, as they include few women and no children. (Still, the new findings echo those from the two pediatric-admissions studies.) Also, like many medical centers, the VA has a policy to test every inpatient for COVID, but this is not a universal practice. Lastly, most of the data—even from the patients admitted in 2021—derive from the phase of the pandemic before Delta became widespread, and it’s possible that the ratios have changed in recent months. The study did run through June 30, however, when the Delta wave was about to break, and it did not find that the proportion of patients with moderate to severe respiratory distress was trending upward at the end of the observation period.
President Trump's COVID-19 Treatments & Medications

President Trump's Medications at Walter Reed Medical Center: Remdesirvir, Regeneron, Zinc, Vitamin D, Famotidine, Melatonin.
Trump's Symptoms were fever and cough.

Remdesivir Anti-Inflamatory

Regeneron Antibody
Subscribe to:
Posts (Atom)
Popular Posts (All Time)
-
 Table of Contents Introduction: Stress, Smoking, and Health The Normotim Effect: A New Hope in Stress Management Lithium Ascorbate:...
Table of Contents Introduction: Stress, Smoking, and Health The Normotim Effect: A New Hope in Stress Management Lithium Ascorbate:... -
 The coronavirus disease (COVID-19) pandemic has been linked to mental health issues related to disease-induced morbidity and mortality and ...
The coronavirus disease (COVID-19) pandemic has been linked to mental health issues related to disease-induced morbidity and mortality and ... -
 Former Hunter Biden business partner Tony Bobulinski has confirmed that an email published in the New York Post's bombshell exposé is ...
Former Hunter Biden business partner Tony Bobulinski has confirmed that an email published in the New York Post's bombshell exposé is ... -
A group of virologists in February 2020 published a letter in The Lancet stating they “overwhelmingly conclude that this coronavirus origina...
-
SAMPLE LETTER BELOW 🚨🚨🚨 The secret is NOT to refuse the Jabb.... From a lawyer: If you are being forced to Vax in order to keep your job,...
-
 The time is now. As most readers of this substack are now well aware, this is not just about COVID. The Constitution hangs in the balance. P...
The time is now. As most readers of this substack are now well aware, this is not just about COVID. The Constitution hangs in the balance. P... -
Klaus Schwab's World Economic Forum Government & WHO Lies Tucker & Malone Discuss The World Economic Forum & It's Young ...
-
 Comment to ACIP meeting of August 30, 2021 submitted by Steve Kirsch - Executive Director of the COVID-19 Early Treatment Fund stk@treatea...
Comment to ACIP meeting of August 30, 2021 submitted by Steve Kirsch - Executive Director of the COVID-19 Early Treatment Fund stk@treatea... -
 2 Sources for this story below . . . Justin Bieber reveals he has Ramsay Hunt syndrome Twitter suspended the VaccineTruth2 account Want to ...
2 Sources for this story below . . . Justin Bieber reveals he has Ramsay Hunt syndrome Twitter suspended the VaccineTruth2 account Want to ... -
 Crimes Against Humanity - The PCR Test Fraud and COVID-19 will be the Case of the Century Reiner Fuellmich - Update on Court Case & P...
Crimes Against Humanity - The PCR Test Fraud and COVID-19 will be the Case of the Century Reiner Fuellmich - Update on Court Case & P...


