
Who Are All the People Involved With Denying and Lying About the Lab Leak Theory?
The COVID-19 lab leak theory has sparked significant controversy and debate since the early days of the pandemic. While some have advocated for a thorough investigation into the virus's origins, others have denied and potentially misrepresented the possibility of a lab leak. This article explores the key figures and organizations involved in denying and possibly lying about the lab leak theory.
Were Vaccines or Natural Immunity More Effective? - I Asked ChatGPT

Were COVID Vaccines Successful? - ChatGPT response . . .
Mainstream Media Will Cause The Fall of Our Democracy
Mainstream media will cause the fall of our democracy.
— Elon Musk (Parody) (@ElonMuskAOC) June 10, 2023
We must fight it. #CancelMainstreamMedia
A healthy democracy requires an informed and engaged citizenry, diverse media sources, responsible journalism, and critical thinking skills.
Sign Petition FDA To Investigate Pfizer's Clinical Trial Fraud

Should the FDA investigate Pfizer's clinical trial fraud allegations? Or look the other way?
The Correct Way to Handle the Pandemic

Vaccines
Stop the vaccines now. The current COVID vaccines kill more people than they can possibly save from COVID, even if they were 100% effective so should be taken off the market immediately. For example, the vaccine may kill 117 kids for every kid that is saved from COVID.
The liability exemption is now lifted retroactively. Patients who have been harmed by the COVID vaccines can now sue the drug company for damages up to $100M per case of fatality or disability.
Every post-vaccination ailment, affliction and death appearing within 4 weeks of vaccination that appears at a rate of 10X or more vs. baseline should be attributed to the vaccine unless and until proven otherwise, by irrefutable evidence, with costs of all diagnostic procedures to be born by the pharmaceutical manufacturer.
For future approved vaccines, informed consent provide shall include any and all symptoms that are elevated in VAERS by 10X or more over “baseline” reporting rates.
For future approved vaccines, require autopsies for anyone who dies within 2 weeks of getting the vaccine. The autopsy reports should be posted in a public database with Names and other PHI related data redacted
Failure to file a VAERS report for anyone who dies within 30 days of COVID vaccination shall be liable to a fine of $100,000 per incident.
Informed consent
If for some reason, we couldn’t stop the vaccine, then everyone should be required to read and sign an informed consent prior to getting vaccinated. Here are some options:
COVID vaccine informed consent form
Family Financial Disclosure Form for Covid-19 Injections
Masks
Instruct public health officers to recommend that businesses post signs saying WARNING: face masks are NOT recommended. They have not been shown to stop COVID and mask wearing may be harmful to your health.
Fairness
There should be no restrictions whatsoever placed on any person who has recovered from a COVID infection since these people cannot transmit future infections. So any sort of testing requirement shall not apply to these people.
Vaccinated and unvaccinated people should be treated the same way since they are equally likely to be infected or spread COVID. So if there is a testing protocol, it must treat vax and unvaxed the same. Same is true for hospitalized patients: there shouldn’t be a separate facility for vaxed vs. unvaxed: they should be treated the same way.
Lockdowns
Lockdowns for COVID are now illegal. COVID is endemic. We are all going to get it sooner or later. So let’s just get it over with and move on. Once you are infected, treat with early treatment and now you are unable to transmit any subsequent re-infection to others.
Mandates
It shall be illegal to coerce anyone to get any vaccination of any type. That goes for military, employer, school, etc. mandates. Vaccination shall be solely up to the individual. People should never be threatened with termination for not being vaccinated. This is especially silly for a vaccine which is toxic and relatively ineffective.
It shall be illegal for any organization to require anyone to wear a mask. Mask wearing should be completely at the option of the wearer. For people who are convinced they work, fine, go wear the mask knowing you will be protected (even though you won’t be).
Inadequately tested drugs
Newly approved drugs with less than a 1 year safety record shall be so labelled by the drug manufacturer in a prominent place that the long-term effects of the drug are unknown.
Early treatment
Put all early treatment protocols with a 95% or higher hospitalization and/or death reduction in clinical practice in hospitalization on a list of recommended treatments in the NIH COVID treatment guidelines
Any drug with at least one positive Phase 3 result (effect size 20% or better) or at least one published systematic-review and meta analysis for use against COVID shall be listed as recommended on the NIH treatment guidelines.
Supplements with a 20% effect size or greater in clinical trials shall be listed as recommended.
All public health officials shall encourage the public to talk to their doctors about the approved early treatment drug / supplement protocols listed on the NIH website.
The public should be encouraged to have on hand drugs for at least one of the early treatment drug / supplement protocol.
Doctors shall comply with patient requests for medications to be administered if there is a sound scientific basis for the request and no sound scientific basis for denying the request. Physicians who ignore this are subject to having their license to practice revoked.
Right to medicine
Revoke the license of any pharmacist who refuses to fill a prescription for an off-label drug where 1) there is clear scientific evidence of a benefit OR 2) where the medication is prescribed in dosages that have been shown to be safe (e.g., dosages approved for the labelled use). This allows a pharmacist to act as a double-check on a physician’s prescription (e.g., to avoid typos, etc) but keeps the pharmacist from second-guessing the prescription.
Scientific integrity
Any publisher who revokes or causes publication delay of a scientific paper without a scientific reason, shall be liable for damages to the author of $100,000 per day.
Scientists can, for good cause, publish papers anonymously (the journal will know). This protects research groups from retribution for publishing “unpopular” science such as confirming the Gundry study. See my article about the Gundry study confirmation where the science was suppressed because the authors were afraid of losing grant money.
Social distancing
There needs to be clear scientific evidence whether this is effective or not. In general, people should make their own personal choice on this. I wish there was a paper showing the effect on transmission versus distance. 6 feet seems a bit too contrived to make me comfortable it is the “right” number people should pay attention to. Where is the science here????
Hospitals
Deliberately mislabeling a death that wasn’t caused by COVID as a COVID death shall be subject to criminal prosecution and a minimum sentence of 10 years in prison.
Halt the use of remdesivir for hospitalized patients. It doesn’t work and it is basically killing people.
Hospitals shall comply with patient requests for medication if there is a clear rationale for the request and a lack of any data showing that the medication is likely to cause more harm than benefit.
Medical free choice
Doctors shall comply with patient requests for FDA approved medications to be administered which are supported by scientific data unless there is a more compelling scientific basis to deny the request.
Hospitals who fire healthcare workers for speaking out (whistleblowers) shall be subject to a private right of action to recover 10 years of wages per incident.
Spreading misinformation about masking and COVID vaccines
Any doctor who tells a patient that the vaccines are “safe and effective” or that cloth or surgical masks can stop COVID shall be called to show the scientific proof of this and lacking such proof shall his license revoked for spreading medical misinformation that can cause patient harm.
Censorship
Any person who is suspended by a social network for communicating truthful scientific data and opinions shall have a private right of action to recover statutory damages of $10,000 per day for ever day the person is suspended.
Any person whose social network post (text or video) is not false and misleading but is erroneously labelled false and misleading is entitled to sue the platform for $10,000 per day that the post is mislabeled or removed by the social network.
Accountability
Criminal prosecution against FDA, CDC, and NIH leaders who are suppressing the science in favor of the narrative. I can assure you, these people are corrupt. It is obvious to anyone with a brain who looks objectively at the data (such as this brilliant article by Josh Guetzkow, Ph.D. Yet the CDC and FDA cannot find a single safety signal? Give me a break. Nobody in Congress is interested in pursuing.
Today, CDC employees like John Su at the CDC, don’t have to answer a single question from the public. Neither do the outside committee members. Instead of a public speaking portion, the public should have the right to ask question of people who are sitting on these committees or make invited presentations. Today we have nothing. None of these people have to answer a single question and even with a million dollar incentive will not sit down for an interview. I wonder what they are so afraid of?
Summary
That’s my list. Not exhaustive, but you get the idea. We need to stop treating this virus like it is radioactive. There are many safe protocols for treating COVID and once recovered, the patient is always better off than if they were vaccinated.
Treating COVID with early treatments of a cocktail of repurposed drugs is the right approach. Vaccination with an unsafe, leaky vaccine in the middle of a pandemic is a recipe for disaster. We need to get off this treadmill ASAP.
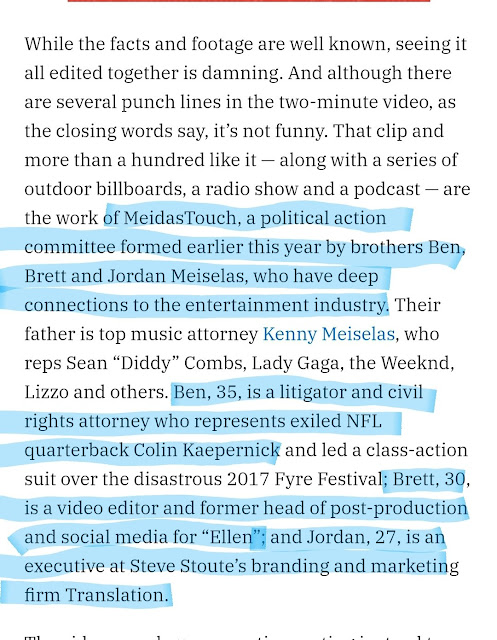
Who Are Ben, Brett and Jordan Meiselas Brothers - Meidas Touch?
Doctor Angelique Coetzee Who Discovered Omicron Was Pressured Not To Reveal It's Mild

When asked if it's true, Coetzee replied: "I was told not to state publicly that it was a mild illness. I have been asked to refrain from making such statements and to say that it is a serious illness. I declined." (translated).
"What does that mean?" replied Welt.
"I am a clinician and based on the clinical picture there are no indications that we are dealing with a very serious disease. The course is mostly mild. I'm not saying you won't get sick if you're mild.
"The definition of mild Covid-19 disease is clear, and it is a WHO definition: patients can be treated at home and oxygen or hospitalization is not required," she said, adding: "A serious illness is one in which we see acute pulmonary respiratory infections: people need oxygen, maybe even artificial respiration. We saw that with Delta - but not with Omikron. So I said to people, "I can't say it like that because it's not what we're seeing.""
When asked why she was prevented from telling the truth, Coetzee said "They tried, but they didn't make it."
"What I said at one point – because I was just tired of it – was: In South Africa this is a mild illness, but in Europe it is a very serious one. That's what your politicians wanted to hear."
According to Coetzee, she wasn't pressured by South African authorities - and was instead criticized by scientists in the UK and Netherlands, who said "How can you explain that it's a mild disease? It's a serious illness. Look at the mutations."
My reports have thrown them off track. In a pandemic, you also have to look at what is happening at the grassroots level. The general practitioners who treat the sick every day must be asked what they experience, how the clinical picture presents itself. -Welt
When Omicron first emerged, Dr. Anthony Fauci played dumb right after praising South African doctors, saying: "The things that we don’t know right now are whether the people who do get infected have a severer form of the disease or whether it’s a light disease or somewhat the same as delta."
Ivermectin Adoption By Country Wordwide Map
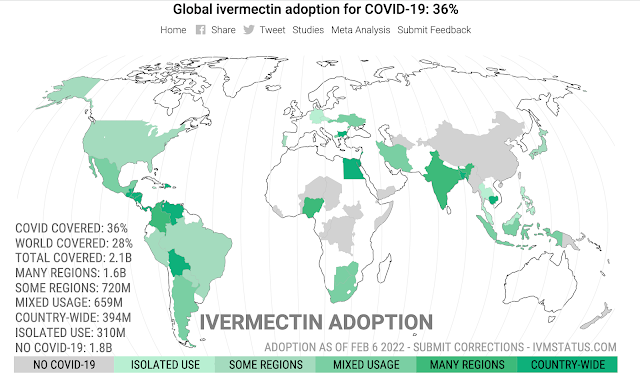
Strictly regular use of ivermectin as prophylaxis for COVID-19 leads to a 90% reduction in COVID-19 mortality rate, in a dose-response manner: definitive results of a prospective observational study of a strictly controlled 223,128 population from a city-wide program in Southern Brazil
Ivermectin is currently used for about 28% of the world’s population. Countries where COVID-19 mortality is close to zero may not have incentive to adopt treatments. When excluding these countries, ivermectin adoption is about 39%. We excluded countries where the cumulative mortality over the preceding month was less than 1 in 1 million.
Western authorities are presenting our choices as either catch covid eventually (because it is so infectious and now spreading everywhere) or take vaccines every three months (according to the latest guidelines), apparently for the indefinite future. They hide and vigorously “omit” the third alternative: the anti-viral path.
Covid, vaccines, or anti-viral. Which is doing better?
Let’s do a scorecard, of official covid deaths per million population [and current daily cases, total, not per capita] on 26 Dec 2021:
Countries that did not close their borders and went to vaccines as soon as possible:
USA – 2,509 [250k]
UK – 2,161 [120k]
Germany – 1,319 [40k]
France – 1,871 [100k]
Canada – 788 [20k]
Italy – 2,265 [50k]
Russia – 2,077 [25k]
Countries that did not close their borders and, after alarming infection, mostly adopted ivermectin:
India – 342 [8k]
Indonesia – 519 [< 1k]
Japan – 146 [< 1k]
Egypt – 205 [< 1k]
Peru – 6,016 (the country hit hardest, until they used ivermectin) [6k]
Columbia – 2,510 [ 3k]
Venezuela – 188 [< 1k]
Nigeria – 14 [4k]
South Africa – 1,502 [20k]
Countries that closed their borders but have recently opened up:
Australia – 84 [10k]
Western Australia – 0.5 [2 cases yesterday, 7 in last few months]
New Zealand – 10 [70]
Vietnam – 314 [16k]
Taiwan – 36 [14] (borders still closed)
Different policies, different health outcomes. Even a bureaucrat could work it out, eventually.
Meanwhile, Pfizer must be very pleased with themselves — producing the most widely used treatment in history!
Vaccines in the west are too big politically to fail — yet they are. There is only so much you can cover up with propaganda and voodoo statistics.
UPDATE: Ivermectin works as well as vaccines, but does not wane and is without the harmful side effects.
The Study:
Background: Previously, we demonstrated that ivermectin use as prophylaxis for COVID-19 was associated with reductions in COVID-19 infection, hospitalization, and mortality rates, and in the risk of dying from COVID-19, irrespective of regularity and accumulated use of ivermectin, in an observational, prospectively obtained data from a strictly controlled city-wide program in a city in Southern Brazil (Itajaí, SC, Brazil) of of medically-based, optional use of ivermectin as prophylaxis for COVID-19.
In this study, our objective was to explore the data obtained from the program to evaluate whether the level of regularity of ivermectin use impacted in the reductions in these outcomes, aiming to determine if ivermectin showed a progressive dose-, regularity-response in terms of protection from COVID-19 and COVID-19 related outcomes.
Materials and methods: This is a prospective observational study of the program mention above, that used ivermectin at a dose of 0.2mg/kg/day for two consecutive days, every 15 days. We obtained and analyzed the data regarding the accumulated dose of ivermectin use, in addition to age and comorbidities, to analyze the patterns of reduction of COVID-19 infection, hospitalization, and mortality rates, and risk of dying from COVID-19, according to the regularity and amount of ivermectin used in a 5-month period.
Following definitions of regularity, we considered as strictly regular subjects that used at least 180mg of ivermectin (180mg = 30 tablets), and as sporadic users subjects that used 60mg (= 10 tablets) or less during the 5-month period.
Comparisons between subjects that did not use ivermectin and these two levels of regularity of ivermectin use were performed. Analysis of the intermediate levels of ivermectin use are present in the supplement appendix of this study. To analyze hospitalization and mortality rates, we utilized the database of COVID-19 infections of all participants, from Itajaí and outside. To analyze COVID-19 infection rate and risk of dying from COVID-19 we utilized the Itajaí city database.
Propensity score matching (PSM) was employed, followed by multivariate adjusted analysis for residual differences (doubly adjusted analysis).
Results:
Of the 7,345 cases of COVID-19, 3,034 occurred in non-users, 1,627 in sporadic users, and 289 in strict users, while the remaining cases occurred in the intermediate levels of ivermectin use. Strict users were older (p < 0.0001) and non-significant higher prevalence of type 2 diabetes and hypertension.
COVID-19 infection rate was 39% lower among strict users [4.03% infection rate; ( p < 0.0001] than in non-users (6.64% infection rate), and non-significant 11% reduction compared to sporadic users (4.54% infection rate) (n = 1,627 in each group; RR, 0.89; 95%CI 0.76 – 1.03; p = 0.11).
Hospitalization rate was reduced by 100% in strict users, compared to non-users and to sporadic users, both before and after Propensity score matching ( p < 0.0001).
After Propensity score matching, hospitalization rate was 35% lower among sporadic users than non-users (RR, 0.65; 95%CI, 0.44 – 0.70; p = 0.03).
In propensity score matched groups, multivariate-adjusted mortality rate was 90% lower in strict users compared to non-users (p = 0.003) and 79% lower than in sporadic users (p = 0.05), while sporadic users had a 37% reduction in mortality rate compared to non-users (p = 0.043).
Risk of dying from COVID-19 was 86% lower among strict users than non-users (p = 0.006) and marginally significant, 72% lower than sporadic users (p = 0.083), while sporadic users had a 51% reduction compared to non-users (p = 0.001).
Conclusion: Non-use of ivermectin was associated with a 10-times increase in mortality risk and 7-times increased risk of dying from COVID-19, compared to strictly regular use of ivermectin in a prospectively collected, strictly controlled population.
A progressive dose-response pattern was observed between level of ivermectin use and level of protection from COVID-19 related outcomes and consistent across different levels of ivermectin use.
The results of this study clearly demonstrate that prophylactic use of ivermectin must be initiated immediately for people in high risk categories in the United States and worldwide. This includes individuals with one or more co-morbidities and the middle aged/elderly. Our “design-to-fail” government funded clinical trials for early treatment and governmental obstructionism regarding life saving treatments to patients must end now.
The CDC chart below for all deaths since the start of the outbreak clearly shows a jump in cases after 50 years old.
However, as the data for deaths per million per age group is not disclosed, so the age for start of prophylaxis has yet to be determined.
As Omicron has less pathogenicity and slightly different disease profile this too could influence what age prophylaxis treatment should begin. But the data are in, prophylactic use of ivermectin saves lives.
A doctor's decision to inform the patient of the 'off-label' status of the prescription is not relevant to the physician's standard of care for an informed consent case.
The FDA has specifically stated that its procedures and requirements have no effect on the practice of medicine and that the FDA does not prohibit doctors from prescribing drugs in an 'off-label' manner.
The FDA's approval of a drug is immaterial to the effectiveness in the drug's 'off-label' use. In fact, prescribing medication in an 'off-label' manner can constitute the standard of care in many cases.
A doctor's duty is to practice medicine and treat his patient, not inform the patient of the FDA's non-medically related labeling. Therefore, doctors should not be branded with the additional duty of disclosing non-pertinent information, such as the FDA's medically irrelevant distinction, to their patients
*It is estimated that 21% of all prescription drugs are prescribed “off-label.”
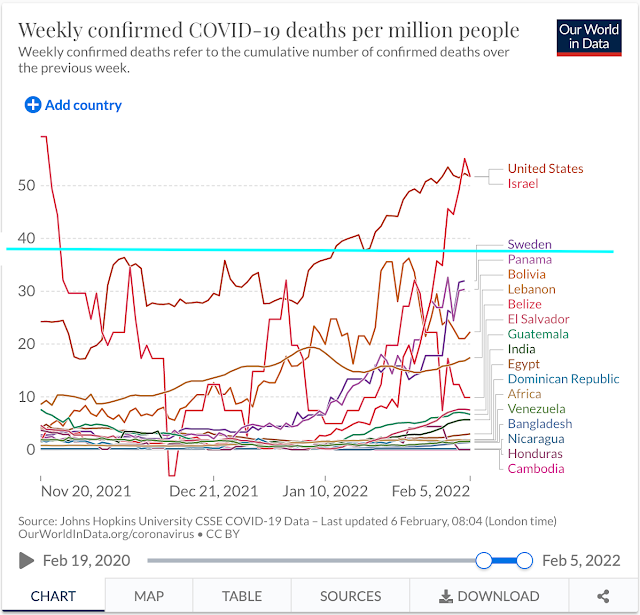
For fun, I took the countries that reportedly use Ivermectin country-wide and compared them to the USA, Israel and Sweden. I chose a three month cut-off, although the results were extended further. I did this because I don’t know when some of the countries began ivermectin use.
Can you guess who now has the highest death rates per million? Yeh -
USA
Israel
Sweden
Notes: I included - India, because although not all regions use Ivermectin - although the most populated due. Likewise Africa - which many nations treat with ivermectin prophylactically and these world maps do not break down Africa by Nations (weirdly imperialistic). I did not include Bulgaria, as although they use ivermectin - their death rate numbers are skewed for other reasons not worth delving into.
There are a lot of confounding variables here. Such as natural immunity, vaccination rates of the elderly and those with co-morbidities, as well as seasonality of the virus, vitamin D3/zinc levels and age of population.
But it is still an interesting snap shot as to where much of the world is right now.
This Gov’t Is the Virus, Media Is How It Spreads, Behavior Is the Pandemic, Common Sense is the Cure
The Government is the virus, the media is how it spreads, people's behavior is how it spreads, and common sense is the cure.
RIP "Trusted News Network" & "Fact Checkers" Dying A Slow Death

How Angry Moms Are Saving Our Democracy From Mass Hypnosis
Popular Posts (All Time)
-
Table of Contents Introduction: Stress, Smoking, and Health The Normotim Effect: A New Hope in Stress Management Lithium Ascorbate:...
-
 The coronavirus disease (COVID-19) pandemic has been linked to mental health issues related to disease-induced morbidity and mortality and p...
The coronavirus disease (COVID-19) pandemic has been linked to mental health issues related to disease-induced morbidity and mortality and p... -
A group of virologists in February 2020 published a letter in The Lancet stating they “overwhelmingly conclude that this coronavirus origina...
-
 Former Hunter Biden business partner Tony Bobulinski has confirmed that an email published in the New York Post's bombshell exposé is i...
Former Hunter Biden business partner Tony Bobulinski has confirmed that an email published in the New York Post's bombshell exposé is i... -
SAMPLE LETTER BELOW 🚨🚨🚨 The secret is NOT to refuse the Jabb.... From a lawyer: If you are being forced to Vax in order to keep your job,...
-
 The time is now. As most readers of this substack are now well aware, this is not just about COVID. The Constitution hangs in the balance. P...
The time is now. As most readers of this substack are now well aware, this is not just about COVID. The Constitution hangs in the balance. P... -
 Comment to ACIP meeting of August 30, 2021 submitted by Steve Kirsch - Executive Director of the COVID-19 Early Treatment Fund stk@treatearl...
Comment to ACIP meeting of August 30, 2021 submitted by Steve Kirsch - Executive Director of the COVID-19 Early Treatment Fund stk@treatearl... -
Klaus Schwab's World Economic Forum Government & WHO Lies Tucker & Malone Discuss The World Economic Forum & It's Young ...
-
 2 Sources for this story below . . . Justin Bieber reveals he has Ramsay Hunt syndrome Twitter suspended the VaccineTruth2 account Want to ...
2 Sources for this story below . . . Justin Bieber reveals he has Ramsay Hunt syndrome Twitter suspended the VaccineTruth2 account Want to ... -
 Crimes Against Humanity - The PCR Test Fraud and COVID-19 will be the Case of the Century Reiner Fuellmich - Update on Court Case & P...
Crimes Against Humanity - The PCR Test Fraud and COVID-19 will be the Case of the Century Reiner Fuellmich - Update on Court Case & P...


