In a significant breakthrough in the fight against cybercrime, the Department of Justice (DOJ) has announced the arrest of 35-year-old YunHe Wang, a Chinese national allegedly responsible for orchestrating a global malware network. This network, known as "911 S5," was purportedly used to steal $5.9 billion in Covid relief funds and was tied to other criminal activities, including child exploitation and bomb threats.

Showing posts with label Money. Show all posts
Showing posts with label Money. Show all posts
Long Covid Action Project - End A Disease That Was Created In A Lab
Long Covid Action Project - End The Disease That Was Created In A Lab
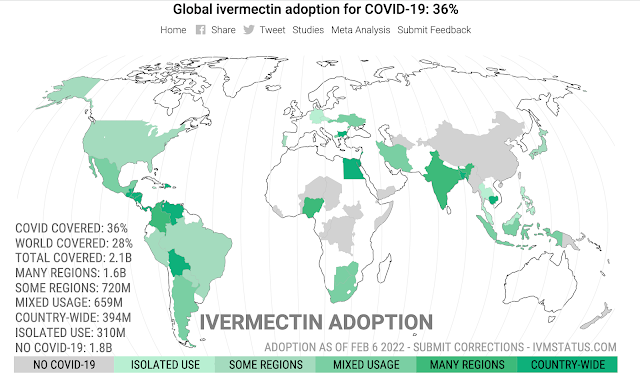
Ivermectin Adoption By Country Wordwide Map
Strictly regular use of ivermectin as prophylaxis for COVID-19 leads to a 90% reduction in COVID-19 mortality rate, in a dose-response manner: definitive results of a prospective observational study of a strictly controlled 223,128 population from a city-wide program in Southern Brazil
Ivermectin is currently used for about 28% of the world’s population. Countries where COVID-19 mortality is close to zero may not have incentive to adopt treatments. When excluding these countries, ivermectin adoption is about 39%. We excluded countries where the cumulative mortality over the preceding month was less than 1 in 1 million.
Western authorities are presenting our choices as either catch covid eventually (because it is so infectious and now spreading everywhere) or take vaccines every three months (according to the latest guidelines), apparently for the indefinite future. They hide and vigorously “omit” the third alternative: the anti-viral path.
Covid, vaccines, or anti-viral. Which is doing better?
Let’s do a scorecard, of official covid deaths per million population [and current daily cases, total, not per capita] on 26 Dec 2021:
Countries that did not close their borders and went to vaccines as soon as possible:
USA – 2,509 [250k]
UK – 2,161 [120k]
Germany – 1,319 [40k]
France – 1,871 [100k]
Canada – 788 [20k]
Italy – 2,265 [50k]
Russia – 2,077 [25k]
Countries that did not close their borders and, after alarming infection, mostly adopted ivermectin:
India – 342 [8k]
Indonesia – 519 [< 1k]
Japan – 146 [< 1k]
Egypt – 205 [< 1k]
Peru – 6,016 (the country hit hardest, until they used ivermectin) [6k]
Columbia – 2,510 [ 3k]
Venezuela – 188 [< 1k]
Nigeria – 14 [4k]
South Africa – 1,502 [20k]
Countries that closed their borders but have recently opened up:
Australia – 84 [10k]
Western Australia – 0.5 [2 cases yesterday, 7 in last few months]
New Zealand – 10 [70]
Vietnam – 314 [16k]
Taiwan – 36 [14] (borders still closed)
Different policies, different health outcomes. Even a bureaucrat could work it out, eventually.
Meanwhile, Pfizer must be very pleased with themselves — producing the most widely used treatment in history!
Vaccines in the west are too big politically to fail — yet they are. There is only so much you can cover up with propaganda and voodoo statistics.
UPDATE: Ivermectin works as well as vaccines, but does not wane and is without the harmful side effects.
The Study:
Background: Previously, we demonstrated that ivermectin use as prophylaxis for COVID-19 was associated with reductions in COVID-19 infection, hospitalization, and mortality rates, and in the risk of dying from COVID-19, irrespective of regularity and accumulated use of ivermectin, in an observational, prospectively obtained data from a strictly controlled city-wide program in a city in Southern Brazil (Itajaí, SC, Brazil) of of medically-based, optional use of ivermectin as prophylaxis for COVID-19.
In this study, our objective was to explore the data obtained from the program to evaluate whether the level of regularity of ivermectin use impacted in the reductions in these outcomes, aiming to determine if ivermectin showed a progressive dose-, regularity-response in terms of protection from COVID-19 and COVID-19 related outcomes.
Materials and methods: This is a prospective observational study of the program mention above, that used ivermectin at a dose of 0.2mg/kg/day for two consecutive days, every 15 days. We obtained and analyzed the data regarding the accumulated dose of ivermectin use, in addition to age and comorbidities, to analyze the patterns of reduction of COVID-19 infection, hospitalization, and mortality rates, and risk of dying from COVID-19, according to the regularity and amount of ivermectin used in a 5-month period.
Following definitions of regularity, we considered as strictly regular subjects that used at least 180mg of ivermectin (180mg = 30 tablets), and as sporadic users subjects that used 60mg (= 10 tablets) or less during the 5-month period.
Comparisons between subjects that did not use ivermectin and these two levels of regularity of ivermectin use were performed. Analysis of the intermediate levels of ivermectin use are present in the supplement appendix of this study. To analyze hospitalization and mortality rates, we utilized the database of COVID-19 infections of all participants, from Itajaí and outside. To analyze COVID-19 infection rate and risk of dying from COVID-19 we utilized the Itajaí city database.
Propensity score matching (PSM) was employed, followed by multivariate adjusted analysis for residual differences (doubly adjusted analysis).
Results:
Of the 7,345 cases of COVID-19, 3,034 occurred in non-users, 1,627 in sporadic users, and 289 in strict users, while the remaining cases occurred in the intermediate levels of ivermectin use. Strict users were older (p < 0.0001) and non-significant higher prevalence of type 2 diabetes and hypertension.
COVID-19 infection rate was 39% lower among strict users [4.03% infection rate; ( p < 0.0001] than in non-users (6.64% infection rate), and non-significant 11% reduction compared to sporadic users (4.54% infection rate) (n = 1,627 in each group; RR, 0.89; 95%CI 0.76 – 1.03; p = 0.11).
Hospitalization rate was reduced by 100% in strict users, compared to non-users and to sporadic users, both before and after Propensity score matching ( p < 0.0001).
After Propensity score matching, hospitalization rate was 35% lower among sporadic users than non-users (RR, 0.65; 95%CI, 0.44 – 0.70; p = 0.03).
In propensity score matched groups, multivariate-adjusted mortality rate was 90% lower in strict users compared to non-users (p = 0.003) and 79% lower than in sporadic users (p = 0.05), while sporadic users had a 37% reduction in mortality rate compared to non-users (p = 0.043).
Risk of dying from COVID-19 was 86% lower among strict users than non-users (p = 0.006) and marginally significant, 72% lower than sporadic users (p = 0.083), while sporadic users had a 51% reduction compared to non-users (p = 0.001).
Conclusion: Non-use of ivermectin was associated with a 10-times increase in mortality risk and 7-times increased risk of dying from COVID-19, compared to strictly regular use of ivermectin in a prospectively collected, strictly controlled population.
A progressive dose-response pattern was observed between level of ivermectin use and level of protection from COVID-19 related outcomes and consistent across different levels of ivermectin use.
The results of this study clearly demonstrate that prophylactic use of ivermectin must be initiated immediately for people in high risk categories in the United States and worldwide. This includes individuals with one or more co-morbidities and the middle aged/elderly. Our “design-to-fail” government funded clinical trials for early treatment and governmental obstructionism regarding life saving treatments to patients must end now.
The CDC chart below for all deaths since the start of the outbreak clearly shows a jump in cases after 50 years old.
However, as the data for deaths per million per age group is not disclosed, so the age for start of prophylaxis has yet to be determined.
As Omicron has less pathogenicity and slightly different disease profile this too could influence what age prophylaxis treatment should begin. But the data are in, prophylactic use of ivermectin saves lives.
A doctor's decision to inform the patient of the 'off-label' status of the prescription is not relevant to the physician's standard of care for an informed consent case.
The FDA has specifically stated that its procedures and requirements have no effect on the practice of medicine and that the FDA does not prohibit doctors from prescribing drugs in an 'off-label' manner.
The FDA's approval of a drug is immaterial to the effectiveness in the drug's 'off-label' use. In fact, prescribing medication in an 'off-label' manner can constitute the standard of care in many cases.
A doctor's duty is to practice medicine and treat his patient, not inform the patient of the FDA's non-medically related labeling. Therefore, doctors should not be branded with the additional duty of disclosing non-pertinent information, such as the FDA's medically irrelevant distinction, to their patients
*It is estimated that 21% of all prescription drugs are prescribed “off-label.”
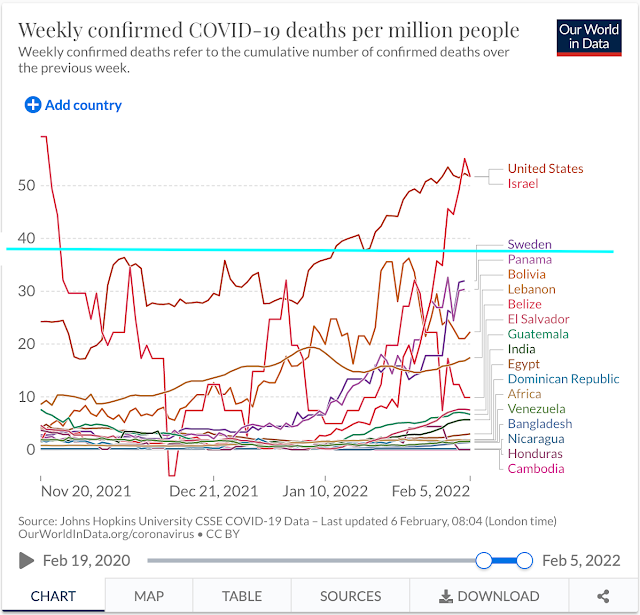
For fun, I took the countries that reportedly use Ivermectin country-wide and compared them to the USA, Israel and Sweden. I chose a three month cut-off, although the results were extended further. I did this because I don’t know when some of the countries began ivermectin use.
Can you guess who now has the highest death rates per million? Yeh -
USA
Israel
Sweden
Notes: I included - India, because although not all regions use Ivermectin - although the most populated due. Likewise Africa - which many nations treat with ivermectin prophylactically and these world maps do not break down Africa by Nations (weirdly imperialistic). I did not include Bulgaria, as although they use ivermectin - their death rate numbers are skewed for other reasons not worth delving into.
There are a lot of confounding variables here. Such as natural immunity, vaccination rates of the elderly and those with co-morbidities, as well as seasonality of the virus, vitamin D3/zinc levels and age of population.
But it is still an interesting snap shot as to where much of the world is right now.
Massive Private Equity Companies Like Black Rock & Vanguard Control Our World
Watch 51 minutes into this video where Robert Malone discusses this massive investment capital that is driving destructive Government decision-making and big pharma corruption.
Consolidation of capital is no longer constrained by a nation-state. These massive private equity companies now control the World and all they care about is the return on investment. They control all decisions in Government and the Federal Reserve. They have war game tools to train politicians.
We call this Stakeholder Capitalism.
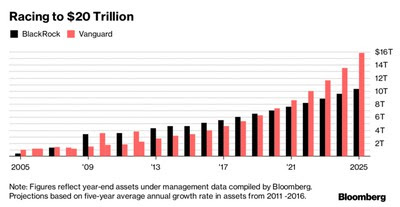


This was 2013 over 8 years ago!
Few people are as qualified to comment on the course of the COVID pandemic and the mass vaccination campaign as Dr. Malone. In this important interview, he shares his unique and deep insights on matters of critical national and international importance
In an exclusive and explosive one-hour interview with Veronika Kyrylenko of The New American, pioneering mRNA scientist Dr. Robert Malone explains the intensely corrupt workings of the government regulatory bodies that have mismanaged the pandemic, discusses the problems with the vaccine program and delves into potentially explosive and game-changing revelations about the shady origins of the Covid-19 pandemic in Wuhan, China.
Who is Dr. Robert Malone? While working at the Salk Institute in 1988, Dr. Malone discovered important findings about in-vivo and in-vitro RNA transfection. He continued his work on the technology a year later at the biopharma start-up Vical where he conducted additional experiments. According to his bio, “The mRNA, constructs, reagents were developed at the Salk institute and Vical by Dr. Malone.” His research has also included important work on DNA vaccines. In addition to his fundamental work developing mRNA and DNA vaccine technology, Malone is also a medical doctor. According to his bio, Dr. Malone “received his medical training at Northwestern University (MD) and Harvard University (Clinical Research Post Graduate) medical school, and in Pathology at UC Davis."
Few people are as qualified to comment on the course of the COVID pandemic and the mass vaccination campaign as Dr. Malone. In this important interview, he shares his unique and deep insights on matters of critical national and international importance.
Still Loaded With Antibodies 1 Year Later After Covid 19 Infection

SEE OTHER TEST RESULTS BELOW
Why Is Natural Immunity Still Being Ignored By The Corrupt Government & Corporate Media?
Blood test results from Labcorp show an unvaccinated family of four people still have antibodies 1 year later after infection. Family of people with ages ranging from 12-48 still are loaded with antibodies.
Can this family get a vaccine mandate exemption?
Our grossly corrupt FDA and Government Advises Against Use of SARS-CoV-2 Antibody Test Results. For one reason only? $MONEY$
Here is the language used by the criminals running the CDC. All eligible people should be vaccinated, including unvaccinated people who have previously been infected and have detectable antibodies.
Numerous immunologic studies (NO STUDIES LINKED?) have consistently shown that vaccination of individuals who were previously infected enhances their immune response, and growing epidemiologic evidence indicates that vaccination following infection further reduces the risk of subsequent infection, including in the setting of increased circulation of more infectious variants.
CDC Website Shows Possible Myocarditisp Side Effects From Those Previously Infected
Risk of an MIS-like illness or the known risks of COVID-19 vaccination such as the rare risk of myocarditis following COVID-19 vaccination for people who meet the following criteria:
- Clinical recovery has been achieved, including return to normal cardiac function;
- It has been ≥90 days since their diagnosis of MIS-C;
- They are in an area of high or substantial community transmission of SARS-CoV-2, or otherwise have an increased risk for SARS-CoV-2 exposure and transmission; and
- Onset of MIS-C occurred before any COVID-19 vaccination.
People diagnosed with MIS-C or MIS-A after COVID-19 vaccination
In the rare instance of a person developing MIS-C, MIS-A, or a similar clinical illness after receipt of a COVID-19 vaccine, referral to a specialist in infectious diseases, rheumatology, or cardiology should be considered. Because MIS-C and MIS-A are conditions known to occur with SARS-CoV-2 infection, these individuals should be assessed for laboratory evidence of current or prior SARS-CoV-2 infection. Healthcare and public health professionals should also consider requesting a consultation from the Clinical Immunization Safety Assessment COVIDvax project. In addition, all illnesses consistent with MIS-C or MIS-A occurring in persons who received any COVID-19 vaccine should be reported to VAERS.
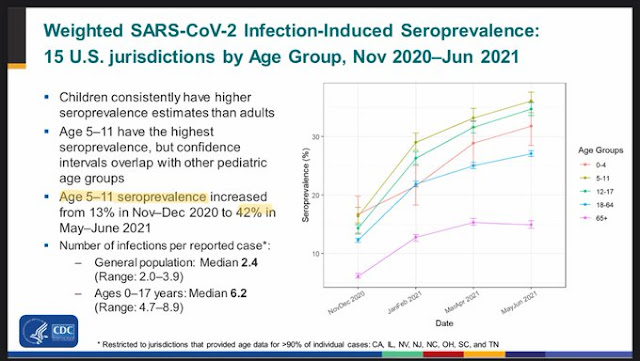
FDA today: 42% of children 5-11 have natural immunity



Who Are The 'Disinformation' Enemies of Truth?
The only way to know who your enemy is in the age of disinformation is to follow the money.
China's Wuhan laboratory is owned by GlaxoSmithKline which owns Pfizer the company that makes the vaccines. Dr. Fauci funded the research at the Wuhan lab through NIH. GlaxoSmithKline is managed by the Private Equity finance division of Black Rock which manages the finances of Open Foundation Group for George Soros which manages the French Accent Group. Soros owns the German company that built the Wuhan laboratory which was bought by the German Alliance which has Vanguard as a shareholder. Black Rock, Vanguard and Alliance control the central banks and also have a large stake in Microsoft where Bill Gates is the Chairman. Bill Gates is a shareholder of Pfizer and BioNTech and a sponsor of the World Health Organization.
Over the past two decades, the Bill and Melinda Gates Foundation has donated “a bit more than $10 billion” into mainly three groups: the Global Alliance for Vaccines and Immunization, the Global Fund to Fight AIDS, Tuberculosis and Malaria, and the Global Polio Eradication Initiative.

Dr. Pierre Kory Treated 200 Members of Congress with Ivermectin
Dr. Pierre Kory treated 200 members of Congress with Ivermectin

GoFundMe Takes Down Campaign For Litigation Over Vax Mandate

The company now insists that it will only allow people to gather on the site if it believes their views are true and correct.
However, it was still surprising to see the site takedown a fundraising account for litigation against vaccine mandates.
The effort of former nurse Jennifer Bridges was simply to get such matters before the courts, which can be the ultimate authority on what is “misinformation.”
GoFundMe however blocked people from contributing to the litigation.
Bridges is a former registered nurse at Houston Methodist hospital who was fired after refusing to comply with the hospital’s vaccine requirement. She raised more than $180,000 for her lawsuit before being shut down under the company’s “misinformation” policy.
Heidi Hagberg, a spokesperson for GoFundMe, said in a statement to Business Insider that “when our team initially reviewed the fundraiser, it was within our terms of service as the funds were for legal fees to fight vaccine mandates. The fundraiser has since been updated to include misinformation which violates our terms of service.”
What is striking about this latest ban is that the courts are the place for such claims to be weighed in a neutral and dispassionate forum. “Misinformation” can be addressed by judges after both sides are allowed to present evidence. Bridges’ lawsuit was dismissed in June, Bridges’ attorneys appealed the decision. We should all favor such reviews. Indeed, if GoFundMe believes that Bridges is wrong, it should invite further judicial review to establish a clear record on such issues.
GoFundMe admits to having taken down “hundreds” of fundraisers that included statements of “misinformation related to vaccines.”
I do not agree with the arguments against the vaccine. I and my family are vaccinated. However, I am equally concerned with avoiding the growing virus of censorship. In the last few years, we have seen an increasing call for private censorship from Democratic politicians and liberal commentators. Faculty and editors are now actively supporting modern versions of book-burning with blacklists and bans for those with opposing political views. The most chilling aspect of this story is how many on the left applaud such censorship. A new poll shows roughly half of the public supporting not just corporate censorship but government censorship of anything deemed “misinformation.”
Free speech can be its own disinfectant for bad speech.
GoFundMe is a private company and can impose such rules on users. However, it is an act of censorship and it is a denial of free speech by a corporation.
In this case, the company is preventing its site from being used to raise money to allow courts to review the factual and legal basis for these claims — a curious effort for a company that claims to be fighting “misinformation.”
GoFundMe takes down fundraiser for anti-vaccine mandate lawsuit
— NNYLiberty (@NNYLiberty) October 8, 2021
The fundraiser by former Houston Methodist nurse Jennifer Bridges had brought in more than $180,000 by the time it was removed.https://t.co/unwg945ngt pic.twitter.com/1UV3lfYEnM
Almost 50% of Hospitalized with COVID-19 Had Mild or Asymptomatic Cases
div class="separator" style="clear: both; text-align: center;">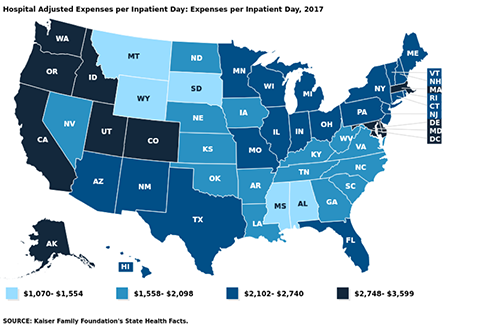

US hospitals typically spend $2,424/day to provide inpatient care. Are hospitalizations another federal money grab?

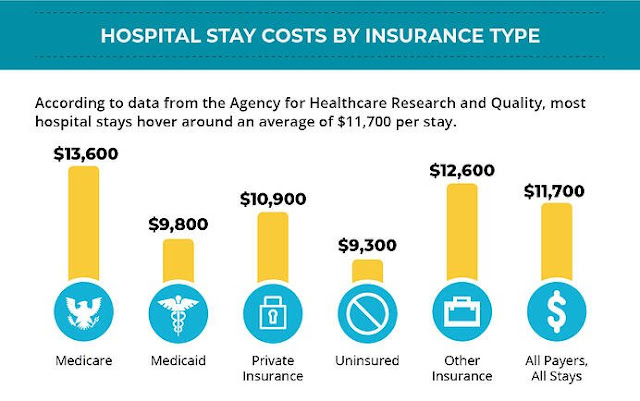
Hospital Stay Costs by Insurance Type
A new study suggests that almost half of those hospitalized with COVID-19 have mild or asymptomatic cases.
Researchers from Harvard Medical School, Tufts Medical Center, and the Veterans Affairs Healthcare System took on the task of trying to figure out how serious Covid cases were in those hospitalized, and how many people counted as Covid hospitalizations were actually in the hospital for Covid, versus getting a Covid test after being admitted for something else.
The study "analyzed the electronic records for nearly 50,000 COVID hospital admissions at the more than 100 VA hospitals across the country," The Atlantic wrote. It "checked to see whether each patient required supplemental oxygen or had a blood oxygen level below 94 percent" in order to try and determine if cases met the NIH's threshold for "severe COVID".
What the study found was that from March 2020 to January 2021, 36% of Covid cases in the hospital were mild or asymptomatic. From January 2021 to June 2021, during the Delta variant's spread, that number rose all the way to 48%. For vaccinated hospital patients, the number rose to a stunning 57%.
At least 12,000 Americans have already died from COVID-19 this month, as the country inches through its latest surge in cases. But another worrying statistic is often cited to depict the dangers of this moment: The number of patients hospitalized with COVID-19 in the United States right now is as high as it has been since the beginning of February. It’s even worse in certain places: Some states, including Arkansas and Oregon, recently saw their COVID hospitalizations rise to higher levels than at any prior stage of the pandemic. But how much do those latter figures really tell us?
From the start, COVID hospitalizations have served as a vital metric for tracking the risks posed by the disease. Last winter, this magazine described it as “the most reliable pandemic number,” while Vox quoted the cardiologist Eric Topol as saying that it’s “the best indicator of where we are.” On the one hand, death counts offer finality, but they’re a lagging signal and don’t account for people who suffered from significant illness but survived. Case counts, on the other hand, depending on which and how many people happen to get tested. Presumably, hospitalization numbers provide a more stable and reliable gauge of the pandemic’s true toll, in terms of severe disease. But a new, nationwide study of hospitalization records, released as a preprint today (and not yet formally peer-reviewed), suggests that the meaning of this gauge can easily be misinterpreted—and that it has been shifting over time.
If you want to make sense of the number of COVID hospitalizations at any given time, you need to know how sick each patient actually is. Until now, that’s been almost impossible to suss out. The federal government requires hospitals to report every patient who tests positive for COVID, yet the overall tallies of COVID hospitalizations, made available on various state and federal dashboards and widely reported on by the media, do not differentiate based on the severity of illness. Some patients need extensive medical intervention, such as getting intubated. Others require supplemental oxygen or administration of the steroid dexamethasone. But there are many COVID patients in the hospital with fairly mild symptoms, too, who have been admitted for further observation on account of their comorbidities, or because they reported feeling short of breath. Another portion of the patients in this tally are in the hospital for something unrelated to COVID, and discovered that they were infected only because they were tested upon admission. How many patients fall into each category has been a topic of much speculation. In August, researchers from Harvard Medical School, Tufts Medical Center, and the Veterans Affairs Healthcare System decided to find out.
Researchers have tried to get at similar questions before. For two separate studies published in May, doctors in California read through several hundred charts of pediatric patients, one by one, to figure out why, exactly, each COVID-positive child had been admitted to the hospital. Did they need treatment for COVID, or was there some other reason for admission, like cancer treatment or a psychiatric episode, and the COVID diagnosis was merely incidental? According to the researchers, 40 to 45 percent of the hospitalizations that they examined were for patients in the latter group.
The authors of the paper out this week took a different tack to answer a similar question, this time for adults. Instead of meticulously looking at why a few hundred patients were admitted to a pair of hospitals, they analyzed the electronic records for nearly 50,000 COVID hospital admissions at the more than 100 VA hospitals across the country. Then they checked to see whether each patient required supplemental oxygen or had a blood oxygen level below 94 percent. (The latter criterion is based on the National Institutes of Health definition of “severe COVID.”) If either of these conditions was met, the authors classified that patient as having moderate to severe disease; otherwise, the case was considered mild or asymptomatic.
The study found that from March 2020 through early January 2021—before vaccination was widespread, and before the Delta variant had arrived—the proportion of patients with mild or asymptomatic disease was 36 percent. From mid-January through the end of June 2021, however, that number rose to 48 percent. In other words, the study suggests that roughly half of all the hospitalized patients showing up on COVID-data dashboards in 2021 may have been admitted for another reason entirely, or had only a mild presentation of the disease.
This increase was even bigger for vaccinated hospital patients, of whom 57 percent had mild or asymptomatic disease. But unvaccinated patients have also been showing up with less severe symptoms, on average, than earlier in the pandemic: The study found that 45 percent of their cases were mild or asymptomatic since January 21. According to Shira Doron, an infectious-disease physician and hospital epidemiologist at Tufts Medical Center, in Boston, and one of the study’s co-authors, the latter finding may be explained by the fact that unvaccinated patients in the vaccine era tend to be a younger cohort who are less vulnerable to COVID and may be more likely to have been infected in the past.
Among the limitations of the study is that patients in the VA system are not representative of the U.S. population as a whole, as they include few women and no children. (Still, the new findings echo those from the two pediatric-admissions studies.) Also, like many medical centers, the VA has the policy to test every inpatient for COVID, but this is not a universal practice. Lastly, most of the data—even from the patients admitted in 2021—derived from the phase of the pandemic before Delta became widespread, and it’s possible that the ratios have changed in recent months. The study did run through June 30, however, when the Delta wave was about to break, and it did not find that the proportion of patients with moderate to severe respiratory distress was trending upward at the end of the observation period.
The idea behind the study and what it investigates is important, says Graham Snyder, the medical director of infection prevention and hospital epidemiology at the University of Pittsburgh Medical Center, though he told me that it would benefit from a little more detail and nuance beyond oxygenation status. But Daniel Griffin, an infectious disease specialist at Columbia University, told me that using other metrics for the severity of illness, such as intensive-care admissions, presents different limitations. For one thing, different hospitals use different criteria for admitting patients to the ICU.
One of the important implications of the study, these experts say, is that the introduction of vaccines strongly correlates with a greater share of COVID hospital patients having mild or asymptomatic disease. “It’s underreported how well the vaccine makes your life better, how much less sick you are likely to be, and less sick even if hospitalized,” Snyder said. “That’s the gem in this study.”
“People ask me, ‘Why am I getting vaccinated if I just end up in the hospital anyway?’” Griffin said. “But I say, ‘You’ll end up leaving the hospital.’” He explained that some COVID patients are in for “soft” hospitalizations, where they need only minimal treatment and leave relatively quickly; others may be on the antiviral drug remdesivir for five days, or with a tube down their throat. One of the values of this study, he said, is that it helps the public understand this distinction—and the fact that not all COVID hospitalizations are the same.
But the study also demonstrates that hospitalization rates for COVID, as cited by journalists and policymakers, can be misleading, if not considered carefully. Clearly many patients right now are seriously ill. We also know that overcrowding of hospitals by COVID patients with even mild illness can have negative implications for patients in need of other care. At the same time, this study suggests that COVID hospitalization tallies can’t be taken as a simple measure of the prevalence of severe or even moderate disease, because they might inflate the true numbers by a factor of two. “As we look to shift from cases to hospitalizations as a metric to drive policy and assess the level of risk to a community or state or country,” Doron told me, referring to decisions about school closures, business restrictions, mask requirements, and so on, “we should refine the definition of hospitalization. Those patients who are there with rather than from COVID don’t belong in the metric.”
Among the limitations of the study is that patients in the VA system are not representative of the U.S. population as a whole, as they include few women and no children. (Still, the new findings echo those from the two pediatric-admissions studies.) Also, like many medical centers, the VA has a policy to test every inpatient for COVID, but this is not a universal practice. Lastly, most of the data—even from the patients admitted in 2021—derive from the phase of the pandemic before Delta became widespread, and it’s possible that the ratios have changed in recent months. The study did run through June 30, however, when the Delta wave was about to break, and it did not find that the proportion of patients with moderate to severe respiratory distress was trending upward at the end of the observation period.
Why Isn't Ivermectin Being Used Promoted For Treatment?

BECAUSE IT IS A CHEAP DRUG AND THERE IS NO MONEY IN IT FOR BIG PHARMA
India destroyed covid with Ivermectin in a few months with only a 2% vaccination rate back in May. In those two months, they brought cases and deaths down 97% wherever it was used and gained herd natural immunity, which prevents spread. The vaccines can't do that because they don't prevent spread.
A 97% decline in Delhi cases with Ivermectin is decisive - period. It represents the last word in an epic struggle to save lives and preserve human rights. This graph symbolizes the victory of reason over corruption, good over evil, and right over wrong. It is as significant as David’s victory over Goliath. It is an absolute vindication of Ivermectin and early outpatient treatment. It is a clear refutation of the WHO, FDA, NIH, and CDC's policies of "wait at home until you turn blue" before you get treatment.
Dr. Pierre Kory told the world on December 8, 2020, that Ivermectin "obliterates" this virus. Obliterate means to decimate, demolish, or annihilate. It means to eliminate or destroy all trace, indication, or significance.
This graph shows that Ivermectin, used in Delhi beginning April 20, obliterated their COVID crisis. No one should be able to talk you out of this - not a salesman, a drug company, a television celebrity doc, and certainly not the top doctor for the WHO or the NIH who is paid to do that.
Will you believe this 97% eradication graph, or will you believe the propaganda pitched by the Big Media, Big Pharma, the WHO, and the FDA, who share massive financial conflicts of interest – those who say there is insufficient evidence?
What evidence could be any clearer than a 97% reduction in five weeks? That number is better than the current vaccines and beyond the reach of most medicines.
The WHO cautioned India they were making a mistake by using Ivermectin. They told them it could be dangerous, that there was no evidence it worked. How many lies will you buy before you stand up for the truth?
India, Argentina and Mexico are using this drug successfully to treat!
Dr. Pierre Kory, the chief medical officer of the Front Line COVID-19 Critical Care (FLCCC) Alliance, called the U.S. government’s decision to grant $1.2 billion to develop a drug to combat COVID-19 a “colossal waste of taxpayer money for a drug we don’t need,” especially since ivermectin works so well.
YouTube banned this video
Facebook's COVID Vaccine FactCheck.org Funded By J&J
Facebook's independent fact-checker might not be so independent after all. US Congressman's questioned the partiality, Fact Check dot org, which is supposed to tackle vaccine disinformation because it's indirectly funded by jab manufacturer Johnson & Johnson.
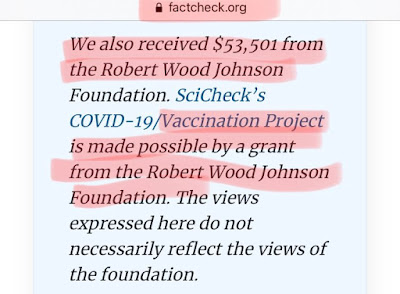
Who pays the paychecks of the fact-checkers? The vaccine fact-checkers at Fact Check dot org, who claim to be independent, are funded by an organization that holds over $1.8 billion of stock in a vaccine company and is run by a former director of the Center for Disease Control.
The fact-checking account responded to accusations by making clear its funding sources. The Robert Wood Johnson Foundation is one of those benefactors billions and owns billions in Johnson & Johnson stock. The foundation's CEO is Richard Besser who is a former acting Director for the Center for Disease Control. Yet Fact Check dot org claims there' no interference in its editorial decisions and the Foundation's views aren't necessarily reflected in its decisions. But author and liberal studies expert Michael Rectenwald believes such connections pose risks to the public.
This absolute collusion on the part of vaccine manufacturers having funded the fact-checkers on social media. So we're actually getting to the point where people's lives are being endangered. We've lost all confidence in social media and our mainstream media entirely. Anything that comes into contradiction with the Leftist's agenda is deemed misinformation. People are now not able to get information about what's best for their health. Including the detriments of the vaccine.
NOTHING TO SEE HERE...
— Thomas Massie (@RepThomasMassie) April 24, 2021
Former director of CDC is now CEO of the foundation that funds FACTCHECK. org’s vaccine fact checking program. Roughly 15% of said foundation’s assets are J&J stock.
Bless your heart if you think factcheck .org is an unbiased source of vaccine information pic.twitter.com/Ijq3sojHmV

Biden Just Caused Vaccines To "Jump The Shark" With A $100 Bribe

President Biden on Thursday called on state and local governments to use funds from his $1.9 trillion American Rescue Plan to offer $100 payments to individuals in order to incentivize coronavirus vaccinations.
The payments would be offered to newly vaccinated Americans to provide “an extra incentive to boost vaccination rates, protect communities, and save lives,” the Treasury Department said in an announcement Thursday afternoon.
“Treasury stands ready to give technical assistance to state and local governments so that they may use the funds effectively to support increased vaccination in their communities, and Treasury will partner with the Department of Health and Human Services throughout this effort,” it said.
Well, it's called exploitation. Prey on those that live week to week and desperately need $. This administration is pathetic, evil, and illegal.
How about instead of a one-time $100 payout to get the injection, why not .gov promise to pay for all related medical bills resulting from adverse reactions to the wu-Flu jab. That would equal somewhere around $100,000 minimum per person.... which might be a better incentive.
$100 isn’t enough
$1,000 isn’t enough
$1,000,000 isn’t enough.
Wait until you need to show proof of vaccination to renew your driver's license, register your car, renew your passport, get a marriage license, and even get your tax refund.
Everything that you need from the government, except to vote..that would be racist. That's why resisting now is so important.
This all reeks of fear and desperation.
Their narrative is coming undone. Too much information is leaking out of their tech-censored bubble.
Meanwhile Pfizer's COVID-19 vaccine generated $7.8 billion in revenue in the second quarter
And all those who already got the vaccine, before the incentive - you are . . . (to be continued)
Jumping the shark is an idiom used to describe the moment of a misguided attempt at generating new publicity for something once, but no longer, widely popular; the attempt serves instead to highlight the irrelevance of what it intends to promote.
20 Divisive Mainstream Media COVID Narratives

20 Mainstream Divisive Covid Narrative Arguments & Counter Arguments
Where Did Covid Start?
- It is not known where Covid originated but the most likely origin is the transmission from an animal to humans
- Covid was most likely created in a lab in China or the US
Deaths
- Covid has killed 600K people in the US
- Covid kills people but far fewer than the official count
Government Response
- Trump botched the Covid 19 response costing many lives
- Almost all officials in government have botched the Covid 19 response, costing many lives
Prevention
- Many deaths were preventable if we’d tested, masked, tracked and locked down better
- Most deaths were preventable if we had investigated and deployed early treatments including vitamin D, zinc, hydroxychloroquine, and ivermectin
Vaccines
- Vaccines are good and have eradicated polio, measles, whooping cough and other diseases
- The Covid 19 vaccines however are not actually vaccines but gene therapy and have not been adequately tested
Vaccine Side Effects
- Vaccines against Covid 19 are safe and effective and have saved many lives with only minor, acceptable adverse reactions
- The Covid 19 vaccines have serious side effects including death and other as yet unknown consequences which are not being investigated and are suppressed by the media
Treatments
- There are no effective treatments for Covid besides the vaccines
- We need to defeat Covid 19 and the best way to do this is through early outpatient treatment with known, effective drugs and known drug protocols for hospitalized patients
How Does It Spread?
- Covid is spread by droplets and aerosols from infected people, both symptomatic and asymptomatic, and can be spread through momentary casual contact both indoors and outdoors
- Covid 19 is primarily spread by aerosols from symptomatic and pre-symptomatic people, mostly in indoor situations with poor ventilation where peoples spend a long time together
Children
- Children and young adults are at risk from Covid and can spread the disease and should take the same precautions and measures as adults
- Children and young adults are at low risk from Covid 19 and need to take fewer precautions and measures but should be treated with drug protocols if infected
Stopping It
- We need to do whatever it takes to defeat Covid including frequent testing, mass vaccination, continued lockdowns, and wearing masks
- Masks, distancing and lockdowns are mostly ineffective
Regulatory Government Agencies
- The best information comes from the CDC, FDA and NIH
- The CDC, FDA, and NIH are largely compromised because of their association with and funding by drug companies
Health & Safety Warnings
- As usual, conspiracy theorists and nut-jobs abound
- The best information comes from front line doctors who actually treat patients and experienced researchers who have no financial interest in big pharma
Mainstream Media Trust
- The mainstream media warns us of the dangers of Covid but unfortunately many do not take these warnings seriously
- The mainstream media is also compromised by their association with big pharma and the government
Vaccine
- Anti-vaxxers are against all vaccines and now also against the Covid vaccines
- People who insist that the vaccines are the only way to fight Covid have believed lies told to them by the MSM from big pharma and a corrupt medical establishment
Censorship
- Anti-vaxxers have believed phony information disseminated by scurrilous, right-wing charlatans
- The truth about Covid is suppressed and labeled conspiracy theory in order to support the mainstream narrative
Who is to blame?
- Anti-vaxxers cost many lives and are the reason Covid still spreads and mutates
- The vaccine narrative has cost many lives and ineffective vaccines are responsible for the continued spread and mutation of Covid
Economy
- Unvaxxed are responsible for continued lockdowns and the further decimation of the economy
- The fallacious mainstream narrative is responsible for all lockdowns and the decimation of the economy
Motivations
- They are selfish, evil and anti-science
- The people who push the mainstream narrative are evil and anti-science; The people who believe this narrative is naive, dogmatic and anti-science
Money & Power
- The Covid response is all about trying to get us back to normal as quickly as possible
- The Covid response is all about money, power, and control
Dr Bryan Ardis - Hospital Protocol Is What Is Murdering "Covid" Flu Patients
Covid Vaccines Mint 9 New Big Pharma Billionaires

At least nine people have become new billionaires since the beginning of the COVID pandemic, thanks to the excessive profits pharmaceutical corporations with monopolies on COVID vaccines are making, The People’s Vaccine Alliance revealed today ahead of a G20 leaders Global Health Summit.
Key members of the G20, who meet tomorrow, including the UK and Germany, are blocking moves to boost supply by ending companies’ monopoly control of vaccine production as COVID-19 continues to devastate lives in countries like India and Nepal where only a tiny fraction of the population has been vaccinated.
Between them, the nine new billionaires, have a combined net wealth of $19.3 billion, enough to fully vaccinate all people in low-income countries 1.3 times. Meanwhile, these countries have received only 0.2 percent of the global supply of vaccines, because of the massive shortfall in available doses, despite being home to 10 percent of the world’s population.
In addition, eight existing billionaires –who have extensive portfolios in the COVID-19 vaccine pharma corporations– have seen their combined wealth increase by $32.2 billion, enough to fully vaccinate everyone in India.
Topping the list of new billionaires are Moderna (MRNA) CEO Stéphane Bancel and Ugur Sahin, the CEO of BioNTech (BNTX), which has produced a vaccine with Pfizer (PFE). Both CEOs are now worth around $4 billion, according to an analysis by the People's Vaccine Alliance, a campaign group that includes Oxfam, UNAIDS, Global Justice Now and Amnesty International.
Senior executives from China's CanSino Biologics and early investors in Moderna have also become billionaires on paper as shares skyrocketed, partly in expectation of profits earned from Covid vaccines, which also bode well for the companies' future prospects. The analysis was compiled using data from the Forbes Rich List.
Moderna's share price has gained more than 700% since February 2020, while BioNTech has surged 600%. CanSino Biologics' stock is up about 440% over the same period. The company's single-dose Covid-19 vaccine was approved for use in China in February.
Activists said the wealth generation highlighted the stark inequality that has resulted from the pandemic. The nine new billionaires are worth a combined $19.3 billion, enough to fully vaccinate some 780 million people in low-income countries, campaigners said.
"These billionaires are the human face of the huge profits many pharmaceutical corporations are making from the monopoly they hold on these vaccines," Anne Marriott, Oxfam's health policy manager, said in a statement. "These vaccines were funded by public money and should be first and foremost a global public good, not a private profit opportunity," she added.
The 9 new vaccine billionaires, in order of their net worth are:
- Stéphane Bancel, Moderna’s CEO (worth $4.3 billion)
- Ugur Sahin, CEO and co-founder of BioNTech (worth $4 billion)
- Timothy Springer, an immunologist and founding investor of Moderna (worth $2.2bn)
- Noubar Afeyan, Moderna’s Chairman (worth $1.9 billion)
- Juan Lopez-Belmonte, Chairman of ROVI, a company with a deal to manufacture and package the Moderna vaccine (worth $1.8 billion)
- Robert Langer, a scientist and founding investor in Moderna (worth $1.6 billion)
- Zhu Tao, co-founder and chief scientific officer at CanSino Biologics (worth $1.3 billion)
- Qiu Dongxu, co-founder and senior vice president at CanSino Biologics (worth $1.2)
- Mao Huihua, also co-founder and senior vice president at CanSino Biologics (worth $1 billion)
The 8 vaccine billionaires who saw their wealth increase are:
Name Role/description $ billions 2021 $ billions 2020
- Jiang Rensheng & family Chair, Zhifei Biological products $ 24.40 $ 7.60
- Cyrus Poonawalla Founder, Serum Institute of India $ 12.70 $ 8.20
- Tse Ping Sinopharm $ 8.90 $ 7.30
- Wu Guanjiang Co-founder, Zhifei Biological products $ 5.10 $ 1.80
- Thomas Struengmann & family Portfolio includes Germany's BioNTech and Uruguay's Mega Pharma $ 11.00 $ 9.60
- Andreas Struengmann & family Portfolio includes Germany's BioNTech and Uruguay's Mega Pharma $ 11.00 $ 9.60
- Pankaj Patel Controls listed company Cadila Healthcare. The company now manufactures drugs to treat Covid-19 such as Remdesivir from Gilead. Its Covid-19 vaccine, ZyCoV-D, is undergoing clinical trials. $ 5.00 $ 2.90
- Patrick Soon-Shiong ImmunityBio - selected for the US federal government's "Operation Warp Speed" to help quickly develop a Covid-19 vaccine. $ 7.50 $ 6.40
Related articles:
COVID-19 Vaccine Passport Scam

Scammers used anything from false masks to COVID-19 scholarships to funeral money to lure victims. They're now concentrating on vaccine passports.
The majority of these ruses are designed to appear to be from the US government. Sylvia, a grandma who fell for the con, received a call saying that now that she'd been vaccinated, she needed to take an online COVID-19 test to ensure the vaccine was functioning before she could acquire a vaccine passport.
"For the first time in more than a year, we're planning a cross-country trip to see our grandchildren," Sylvia remarked. "As a result, I wanted to double-check that we're doing everything we need to do in order to travel."
Sylvia was told that the test would cost her $25 by the con artist. As a result, she provided the fraudster with her bank account number in order to pay for two tests for herself and her husband. The scammer got $500 out of the account instead of $50. When Sylvia reported the event, the bank closed her account.
Texts or emails with links to a testing website, as well as phishing for personal and financial information, are examples of other versions.
It's vital to remember that there is no requirement for post-vaccination testing. There are no online tests available without a sample, and no vaccine passports are necessary. So ignore any unsolicited emails or texts about COVID-19 testing, and hang up on anyone phoning about it.
How to spot a COVID-19 scam:
- Government agencies usually don't communicate through text messages
- Go to the agency's website yourself, without clicking on a link, to verify any information you receive via text or email.
- Ignore instructions to text "STOP" or "NO" to prevent future texts, and don't hit unsubscribe to stop emails. That is a common ploy by scammers to confirm they have an actual, active number.
- Also, check for look-alikes
Be sure to do research and see if a government agency or organization mentioned in a text or email exists. Find contact information and call to see if what you've been told is legitimate.
How Much Money Did J&J Make From COVID Vaccines?

The company is on track to produce 1 billion doses for global distribution by the end of 2021, which would generate up to $10 billion. In August, Johnson & Johnson reached a more than $1 billion agreement with the United States for 100 million doses of its vaccine, with the option to purchase an additional 200 million doses, for $10 per shot. In addition, Johnson & Johnson reached an agreement with the E.U. for up to 400 million doses.
CDC and FDA have recommended a pause in the use of the Johnson & Johnson’s Janssen COVID-19 vaccine in the United States out of an abundance of caution, effective Tuesday, April 13. CDC will convene a meeting of the Advisory Committee on Immunization Practices (ACIP) on Wednesday, April 14, to address this issue. People who have received the J&J/Janssen COVID-19 vaccine within the past three weeks who develop severe headache, abdominal pain, leg pain, or shortness of breath should contact their health care provider.
How Much Does Big Pharma Spend on Advertising & PR?

TV Advertising Spending by Network in 2015 (Not accurate but you get the point)
News used to be separate from entertainment programs. Those rules were changed. New Zealand and the US are the only countries that allow pharmaceutical product ads on TV. Our news outlets are now majority funded by pharma. In another record year for pharma TV ads, more than 70% of advertising is spent by big pharma ($5B).

.
1. AbbVie’s Humira: $375 million
2. Pfizer’s Lyrica: $213 million
3. Pfizer’s Xeljanz: $209 million
4. Eli Lilly’s Trulicity: $183 million
5. Bayer and Johnson & Johnson's Xarelto: $143 million
6. Celgene’s Otezla: $139 million
7. Pfizer and Bristol-Myers Squibb's Eliquis: $136 million
8. Merck’s Keytruda: $107 million
9. Pfizer’s Ibrance: $92 million
10. Boehringer Ingelheim and Eli Lilly's Jardiance: $86 million
11. Otsuka and Lundbeck's Rexulti: $84 million
12. Eli Lilly’s Taltz: $83 million
13. Eli Lilly’s Verzenio: $80.4 million
14. Pfizer’s Prevnar 13: $79.9 million
15. Pfizer’s Eucrisa: $79.7 million
16. Sunovion’s Latuda: $78 million
17. Novo Nordisk’s Victoza: $78 million
18. AstraZeneca’s Farxiga: $75 million
19. Amgen’s Enbrel: $70 million
20. Novartis’ Cosentyx: $64 million
Here is a list of top 50 companies. Why Istn't J&J On This List?
If you watch television for any amount of time, you’re probably going to see a drug commercial that tugs on your heart strings, promises to heal your worst medical conditions, and then a voiceover will quickly gloss over the multitude of side effects in a too-quick-to-understand string of monotone words. Prescription medications are are multi-BILLION dollar industry that’s making not only the pharmaceutical companies tons of money, but also the network television stations. How is this influencing public opinion AND health?
Are you annoyed yet how much these ads are on TV? Equally concerning is that pharmaceutical advertising is banned in just about every country except the United States and New Zealand. And consider this: the average American watches 16 hours of pharmaceutical commercials each year which is more time than they spend with their primary physician. One-third of these people ask their doctors about a drug advertisement and most request a prescription.
Are any these companies responsible for the negative PR campaigns to smear Dr. Judy Mikovitz theory PhD Scientist "A Vaccine Could Be Causing The Covid-19 Pandemic"? All of these debunking articles are trying to discredit Judy's reputation and none of them really are answering the true questions that she raises.

If you enjoyed this article you also might like to read these articles:
Subscribe to:
Posts (Atom)
Popular Posts (All Time)
-
Table of Contents Introduction: Stress, Smoking, and Health The Normotim Effect: A New Hope in Stress Management Lithium Ascorbate:...
-
 The coronavirus disease (COVID-19) pandemic has been linked to mental health issues related to disease-induced morbidity and mortality and p...
The coronavirus disease (COVID-19) pandemic has been linked to mental health issues related to disease-induced morbidity and mortality and p... -
A group of virologists in February 2020 published a letter in The Lancet stating they “overwhelmingly conclude that this coronavirus origina...
-
 Former Hunter Biden business partner Tony Bobulinski has confirmed that an email published in the New York Post's bombshell exposé is i...
Former Hunter Biden business partner Tony Bobulinski has confirmed that an email published in the New York Post's bombshell exposé is i... -
SAMPLE LETTER BELOW 🚨🚨🚨 The secret is NOT to refuse the Jabb.... From a lawyer: If you are being forced to Vax in order to keep your job,...
-
 The time is now. As most readers of this substack are now well aware, this is not just about COVID. The Constitution hangs in the balance. P...
The time is now. As most readers of this substack are now well aware, this is not just about COVID. The Constitution hangs in the balance. P... -
 Comment to ACIP meeting of August 30, 2021 submitted by Steve Kirsch - Executive Director of the COVID-19 Early Treatment Fund stk@treatearl...
Comment to ACIP meeting of August 30, 2021 submitted by Steve Kirsch - Executive Director of the COVID-19 Early Treatment Fund stk@treatearl... -
Klaus Schwab's World Economic Forum Government & WHO Lies Tucker & Malone Discuss The World Economic Forum & It's Young ...
-
 2 Sources for this story below . . . Justin Bieber reveals he has Ramsay Hunt syndrome Twitter suspended the VaccineTruth2 account Want to ...
2 Sources for this story below . . . Justin Bieber reveals he has Ramsay Hunt syndrome Twitter suspended the VaccineTruth2 account Want to ... -
 Crimes Against Humanity - The PCR Test Fraud and COVID-19 will be the Case of the Century Reiner Fuellmich - Update on Court Case & P...
Crimes Against Humanity - The PCR Test Fraud and COVID-19 will be the Case of the Century Reiner Fuellmich - Update on Court Case & P...


